



To book an appointment online please choose from the options below
Normal Structure
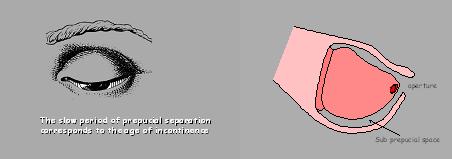
The penis is covered with an outer layer of skin and inner layer, which is in close contact with the tip of the penis “glans”. This is nature’s way of protecting the tip.<
This is the appearance at birth and hence the foreskin will not retract. This situation changes through infancy and childhood and almost all boys by the age of 17 will have a fully retractile foreskin. ( a foreskin that can be pulled back to bare the tip of penis)
Changes through infancy and childhood:
The inner layer of foreskin starts separating from the tip in small areas around the head of the penis. This happens gradually over time, so that some areas are still adherent and some are separated creating small pockets. It is in these areas that the urine collects temporarily causing ballooning which is an entirely normal process.
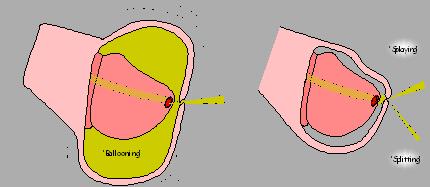
It is important to know that this inner layer of skin also secretes a whitish substance called “smegma” which can collect underneath the foreskin, giving rise to appearances like “pearls”.
You will now be able to understand that when your child passes urine the foreskin may balloon, there may be whitish “smegma” collection and also within this loose foreskin some drops of urine may remain trapped.
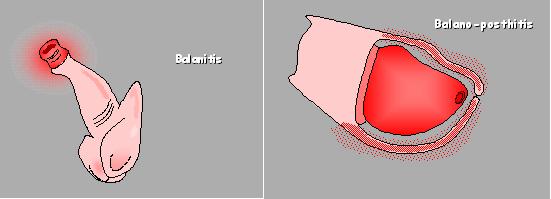
These retained drops of urine and the secretions normally present may invite infection, when the foreskin may become itchy, red and inflammed.
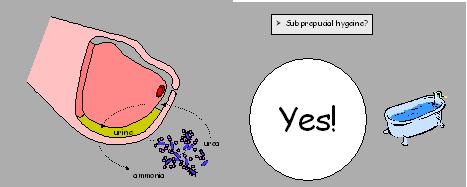
Local hygiene
To avoid this, you, as parent need to monitor and help your child to keep the foreskin clean i.e. towards the end of the bath pull back the foreskin “as much as it can” without using undue force, wash it with soap and water and reposition the foreskin back on the tip of the penis.
If you follow the procedure on a daily basis no further measures will be necessary in the majority of boys.
This means that your boy may have the following:
1 in 150 boys have hypospadias. If the father of the child had hypospadias then the chances are high for his son and higher for a second boy as well.
Dependent on the severity of the problem your boy may be unable to pass urine in the standing position and when older have difficulty in sexual activity. . All of these can be corrected by the repair of hypospadias. The cosmetic appearance of his penis can also be improved.
The operation will be explained to you in further details, discuss any concerns you may have and ask you to sign the consent form for the operation to say you agree. An anaesthetist will also explain to you the general anasesthetic procedure. Your boy may need to stay 1 night in the hospital.
The aim of the operation is to make sure the penis is straight, to move the opening to nearer the tip of the penis, to rearrange the hooded skin to give the appearance like after circumcision. If the hole is further back on the penis the operation may need to be carried out in stages (at least 2 operations) with an interval of 6 to 8 months in between. This will be explained to you by the surgeon.
This is illustrated in the figures below:
Single stage repair of hypospadias:
Two stage repair:
Your boy will be brought back to the ward to recover and may need to stay 1 night in the hospital. He will be able to eat and drink soon after the operation.
He will have a large dressing on his penis and a plastic tube (urinary catheter) will be in place in his newly operated urethra to take the urine away from the site of the operation. Both the dressing and tube will be taken down after 1 week on the ward but your boy does not need to be an in patient for that duration.
Like many operations there are some complications known with this operation but the surgeon doing the operation is experienced and an expert in the field hence the risk is small.
The opening can come back (1 in 15) and the new opening can become narrow (1 in 50). If the opening comes back your boy will need another operation to mend the opening but only after an interval of 6 to 8 months to allow the tissues to heal. If the opening from where he passes urine becomes narrow it will need to be stretched under a general anaesthetic.
Coincidental infection despite the given antibiotics is usually responsive to a change of antibiotic.
Make sure you collect your boy’s medications before going home. He needs at least 4 medicines 1. Oxybutynin this keeps the bladder from being jumpy as the plastic tube drains urine away from the bladder and the bladder is clamped down on the tube irritating it, this is called bladder spasms. 2. Pain killers 3. Lactulose to help him go to toilet easily without the need to strain which may cause discomfort. 4. Antibiotic to prevent infection.
Avoid bathing for 1 week but you may shower him and keep the site of operation dry.
Using double nappies protects from accidental knocks.
If the dressing gets soiled dab any faeces off with a damp cloth
** You need to remember to discontinue oxybutynin 1 day prior to return to the ward for dressing removal so that he will be able to pass urine by squeezing his bladder, oxybutynin relaxes the bladder.
You should contact the hospital if :
Once the dressing is removed the penis looks bruised swollen and unpleasant but this appearance changes with time and in 3 to 4 weeks starts looking like a normal penis.
You will be sent an outpatient appointment to check on your boy’s progress.
I have a complication rate for distal hypospadias following a single stage reapir as follows:
Complication rated for 2 stage repair of which the first stage consists of a preputial graft are as follows:
This is a condition where the penile skin distribution around the shaft(body) of the penis is abnormal. There is usually a deficiency of the skin on the under surface of the penis. The attachment of the skin around the penis is also different giving an appearance that the penis is ‘buried’.
There are other terms used in the literature on this condition as ‘intussusepted foreskin’ and one of the underlying cause put forward is that the end opening of the foreskin is too small or tight.
Whatever the underlyning cause this condition requires treatment as if left alone may lead to complications like inability to pass urine without compressing the ballooned foreskin, local infection and discomfort.
The treatment options may be dependent on the severity are:
The operation involves removal of the thickened inner layer of the foreskin and rearranging of the available skin around the penis.
Sometimes if the skin is deficient to cover the shaft of the penis a skin graft maybe necessary on rare occasions.
A hydrocoele is a fluid filled sac surrounding the testicle and within the scrotum. As the testicle is descending it passes from the back to front in the groin through a muscular canal in doing so carries a lining of the tummy wall with it as a sleeve. This sleeve (connection) usually closes after birth and certainly does so by the age of 2 but in a few boys this happen and the connection persists. This allows the fluid in the tummy around the intestines to flow through this canal into the scrotum surrounding the testicle.
It is very common in newborn boys. Natural resolution takes place by 2 years of age if this fails to happen an operation is needed to cure it.
The scrotum appears swollen like a balloon filled with water. This condition is not painful. Sometimes you may find that the swelling is bigger at the end of the day than the morning when your baby has just woken up, this is due to the fact during the day they are upright and the fluid remains in the scrotum whereas in the morning the fluid may have had a chance to drain back in to the tummy.
Under a general anaesthetic a cut is made in the groin and the sleeve of tummy lining through the fluid comes to the scrotum is carefully separated from the blood supply of the testicle and divided and tied off. The cut is closed. This will be done as a day case which means you will be able to take your child home the same day if all goes well.
The operation will take 30 minutes.
A general anaesthetic risk is small but exists. This will be explained by your child’s anaesthetist who is experienced in giving children a general anaesthetic and dealing with any complication should it arise.
As any other operation there may be some risks like a small blood clot forming in the area and infection but in only a small number of boys.
Your child will be brought back to the ward till he recovers and then allowed home once he feels comfortable. If there are any problems please contact us.
At birth majority but not all boys have 2 testes in the scrotum (skin pouch at the base of the penis) one on each side. This depends on the time of gestation (development) when they are born. If they are born early due to various reasons the testes are still on their way to the scrotum and will get there in a few weeks to months after birth. Commonly it is one testicle that is affected, rarely both may be affected.
In some boys (a small number) despite the fact that they are born at the right time the testes have still not reached the scrotum and could have stopped along the path they follow from the site from where they develop (near the kidneys at the back) to their final destination in the scrotum.
In majority of these boys the testes will eventually reach the scrotum in the first 6 months or so and in the remaining by one year of age.
However if for various reasons the testis has not formed or formed and withered away as it has twisted on itself and cut out its own blood supply obviously the testis will be absent on that side.
As the testes are formed at the back they need to travel from the back to the front through the the groin to finally settle in the srotum.
In some boys the testicle will be in the for much of the time but cannot be felt there because they naturally rise back into the body through fear or cold temperatures. If so there is no cause for concern. However if the testis is permanently in the abdomen, treatment will be needed.
The normal passage in the groin through which the testicle passes from the tummy to the scrotum is not formed. On rare occasions the testicle does not descend due to other problems with the testicles themselves or with the male hormones.
This condition is more common in premature babies. One in 30 boys born at term may be born with undescended testicle and 1 in 70 the testicle remains undescended.
Your doctor will need to examine your baby to determine whether the testicles have truly undescended or whether they have slid back into the body temporarily. As a parent you may check on this by feeling for the testicle at the end of a warm bath.
This is treated with a small operation named ‘orchidopexy’. This involves making a cut in the groin and on the scrotum where the testicle will be anchored, after your baby is anaesthetised. The testis is moved down into the scrotum and the gap is closed. This operation when performed within the first few year of life gives the testicle the best chance to develop normally.
A general anaesthetic risk is small but exists. This will be explained by your child’s anaesthetist who is experienced in giving children a general anaesthetic and dealing with any complication should it arise.
As any other opearation the risk of bleeding and infection are there but in small number of boys. Sometimes despite taking care the testicle may be damaged but this will be obvious a few months later at follow up when your boy will be seen by the surgeon in the outpatient department by comparing it with the opposite testis.
Your child may experience some bruising and soreness in the groin around the cuts. You are advised to give him paracetamol every 4 to 6 hourly. Avoid riding a bicycle for a month. There is no need for the stitches to be removed as they are dissolvable.
Please fill in the form below to send us your enquiry
Second opinion becomes a second chance for patient.
Call Us : 07791 916653








